


Understanding Erectile Dysfunction
Erectile dysfunction (ED) is the inability to achieve or maintain an erection sufficient for satisfactory sexual activity. It affects roughly 30 % of men in the United States, with prevalence rising sharply with age—about half of men over 50 and up to 70 % of those over 70 experience it. The condition also appears in younger men; 8‑15 % of men under 40 report some degree of dysfunction, and it can be an early warning sign of cardiovascular disease, diabetes, or metabolic syndrome. Beyond the physical limitation, ED undermines self‑esteem, intimacy, and quality of life, often leading to anxiety, depression, and relationship strain. Because ED frequently signals health problems, patient education is critical: it encourages men to seek medical evaluation, adopt lifestyle changes that improve vascular health, understand treatment options—including PDE5 inhibitors—and engage partners in open communication. Informed patients are to adhere to therapy, reduce risk factors, and achieve better sexual health outcomes.
Latest Advances in Erectile Dysfunction Treatment

The most recent advances in erectile‑dysfunction care focus on regenerative and non‑invasive options that go beyond traditional oral pills. Low‑intensity shockwave therapy (Li‑ESWT) and low‑intensity pulsed ultrasound are now being used to stimulate new blood‑vessel growth in the penis, often providing lasting improvement for 6‑12 months with minimal side effects. Emerging cellular therapies such as mesenchymal stem‑cell injections and platelet‑rich‑plasma (PRP) infusions aim to repair damaged vascular and nerve tissue, while early‑stage gene‑therapy trials target enhanced nitric‑oxide production. A newer oral agent, udenafil, offers a rapid onset and longer duration compared with older PDE‑5 inhibitors, and the first FDA‑cleared over‑the‑counter topical gel, Eroxon (MED3000), can produce an erection within minutes of application. These cutting‑edge treatments are typically offered in physician‑led regenerative clinics like BeYounger, where personalized, medically supervised protocols are tailored to each patient’s underlying causes and goals. By integrating lifestyle optimization, hormonal assessment, and these innovative therapies, clinicians can address both the vascular and neuro‑muscular components of ED, providing men with a broader toolbox for restoring sexual health.
First‑Line and Best‑Practice Treatment Strategies
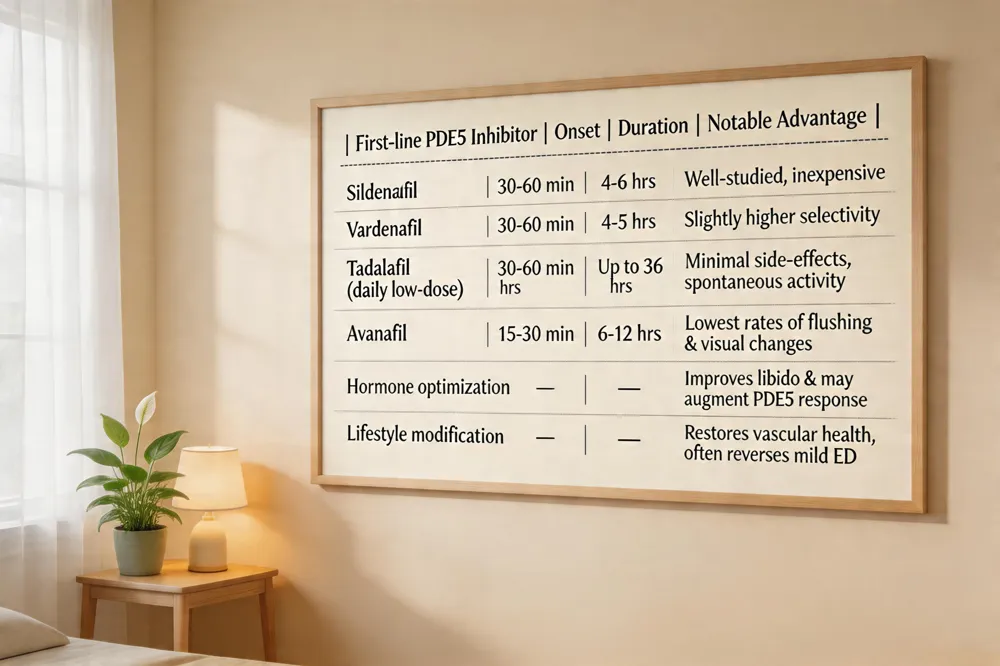 The most effective first‑line therapy for erectile dysfunction (ED) is a phosphodiesterase‑5 (PDE5) inhibitor. FDA‑approved options—sildenafil, vardenafil, tadalafil and avanafil—enhance nitric‑oxide‑mediated smooth‑muscle relaxation, increasing penile blood flow in response to sexual stimulation. Avanafil is noted for the lowest incidence of flushing, headache and visual changes, while low‑dose daily tadalafil often yields minimal side‑effects because steady plasma levels avoid peaks. Hormone optimization is essential when morning testosterone is low; measured low testosterone can be treated with testosterone replacement, which improves libido and may augment PDE5 response. Lifestyle modification is the foundation of any ED plan: regular aerobic exercise (≥150 min/week), a heart‑healthy Mediterranean‑style diet rich in fruits, vegetables, whole grains, lean protein, weight control, smoking cessation and moderate alcohol intake restore vascular health and often restore erections without medication. For men who do not achieve satisfactory results with oral agents, second‑line options include intracavernosal alprostadil injections, vacuum erection devices, penile prosthesis surgery and emerging regenerative therapies such as low‑intensity shockwave, which should be pursued within clinical trials or under specialist supervision.
At‑Home Testing and Early Detection
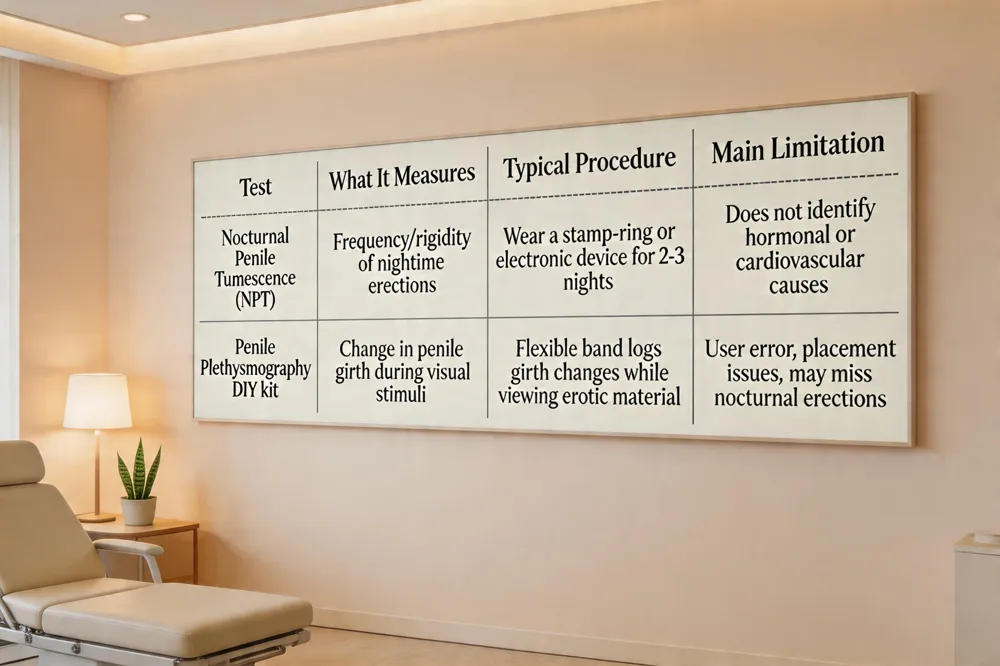
How can I test for erectile dysfunction at home? You can try an at‑home nocturnal penile tumescence (NPT) test, which uses a simple ring of stamps or a small electronic device that records erections that occur while you sleep over several nights. A penile plethysmograph DIY kit is another option; it measures changes in penile girth while you view sexual stimuli, helping to differentiate physical from psychological causes. Both methods can indicate whether you are able to achieve an erection without a partner’s involvement.
Nocturnal penile tumescence testing is valuable because most men experience several erections during REM sleep; a lack of nighttime erections suggests a vascular or neurological problem. Penile plethysmography kits typically involve a flexible band placed around the shaft that logs girth changes in response to erotic material.
Limitations of self‑testing are significant. These tools do not diagnose underlying hormonal, cardiovascular, or medication‑related factors, and results can be affected by user error, poor device placement, or inconsistent sleep patterns. False‑negative or false‑positive findings may lead to delayed professional care. Because erectile dysfunction often reflects broader health issues, a thorough evaluation by a urologist or a physician‑led clinic is essential for accurate diagnosis and a personalized treatment plan.
Vascular Health – The Core Cause of Erectile Dysfunction

The primary driver of erectile dysfunction (ED) is impaired blood flow to the penis, most often caused by vascular disease-guideline). Atherosclerosis narrows the penile arteries, limiting the volume of blood that can fill the corpora cavernosa during sexual arousal. Hypertension, diabetes, and obesity further damage the endothelium and reduce nitric‑oxide availability, compromising vasodilation and smooth‑muscle relaxation. Studies show that men with waist circumferences of 42 inches are 50 % more likely to experience ED than those with a 32‑inch waist. Lifestyle factors such as smoking and excessive alcohol intake accelerate arterial stiffness and oxidative stress, while regular aerobic exercise, a heart‑healthy diet rich in fruits, vegetables, whole grains, and lean protein, and weight management improve endothelial function and restore erectile quality. Pelvic‑floor (Kegel) exercises can augment blood‑trapping mechanisms, but they work best when the underlying vascular system is healthy. Addressing these cardiovascular risk factors—through smoking cessation, blood‑pressure control, glucose management, and a Mediterranean‑style diet—offers a foundational strategy for reversing ED and reducing the risk of future heart disease.
Medication‑Induced Erectile Dysfunction
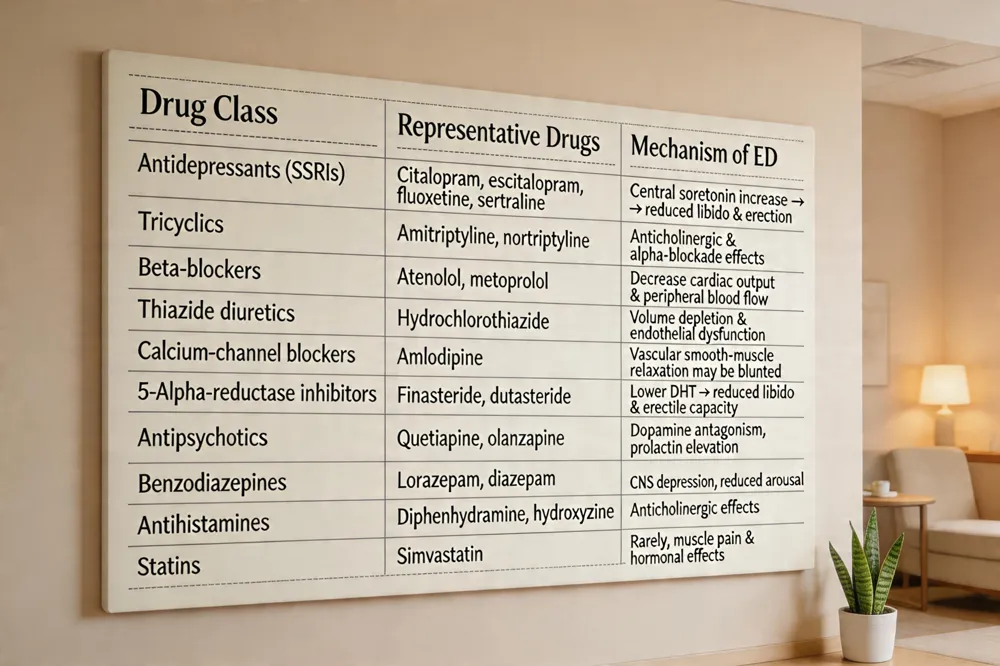
Certain prescription drugs are well‑documented contributors to erectile dysfunction (ED). Antidepressants—especially selective serotonin reuptake inhibitors (SSRIs) such as citalopram, escitalopram, fluoxetine, and sertraline—as well as tricyclic agents, rank among the most frequent offenders. Blood‑pressure medications also play a notable role; beta‑blockers, thiazide diuretics, and some calcium‑channel blockers (e.g., amlodipine) can impair penile blood flow. 5‑Alpha‑reductase inhibitors used for benign prostatic hyperplasia or androgen‑loss (finasteride, dutasteride) are another common cause, often linked to reduced libido and erectile difficulty. Additional culprits include antipsychotics (quetiapine, olanzapine), benzodiazepines, certain antihistamines (diphenhydramine, hydroxyzine), and statins such as simvastatin. FDA adverse‑event data highlight finasteride, dutasteride, amlodipine, paliperidone, citalopram, sertraline, isotretinoin, escitalopram, quetiapine, and simvastatin as the top ten drugs associated with ED. Clinicians should review a patient’s medication list, consider alternatives or dose adjustments, and discuss these side‑effects openly to mitigate the impact on sexual health.
Natural Beverages that Support Erectile Health
Staying well‑hydrated with plain water is the foundation, as dehydration can impair circulation and reduce nitric‑oxide production.
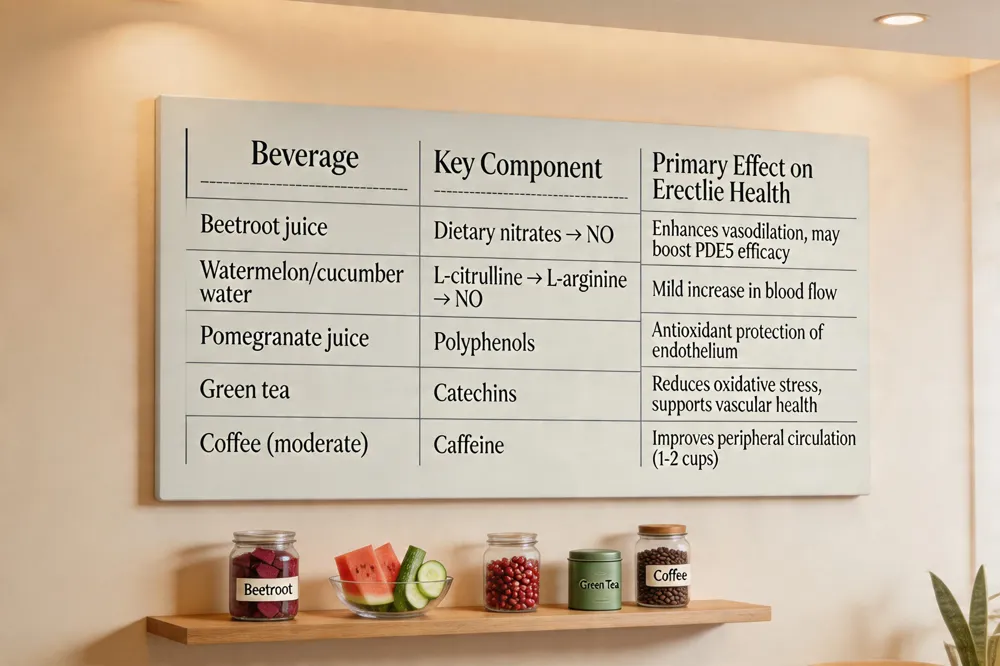
Beetroot juice and nitrates – Beetroot is rich in dietary nitrates, which the body converts to nitric oxide, a key vasodilator that relaxes penile blood vessels and may enhance the effectiveness of PDE5 inhibitors.
Watermelon and cucumber water for L‑citrulline – Both fruits contain L‑citrulline, a precursor that the body turns into L‑arginine and then nitric oxide, providing a mild, sugar‑free boost to blood flow.
Pomegranate and green tea antioxidants – Pomegranate juice supplies polyphenols that protect endothelial cells, while green tea’s catechins reduce oxidative stress, together supporting vascular health essential for erections.
Coffee moderation – Caffeine can improve peripheral circulation when consumed in moderate amounts (1–2 cups daily); excessive intake may increase anxiety and heart rate, potentially offsetting benefits.
These drinks are supportive, not curative, and work best when paired with regular aerobic exercise, a heart‑healthy diet, weight management, smoking cessation, and any prescribed ED therapy.
Self‑Care Strategies to Boost Erectile Function
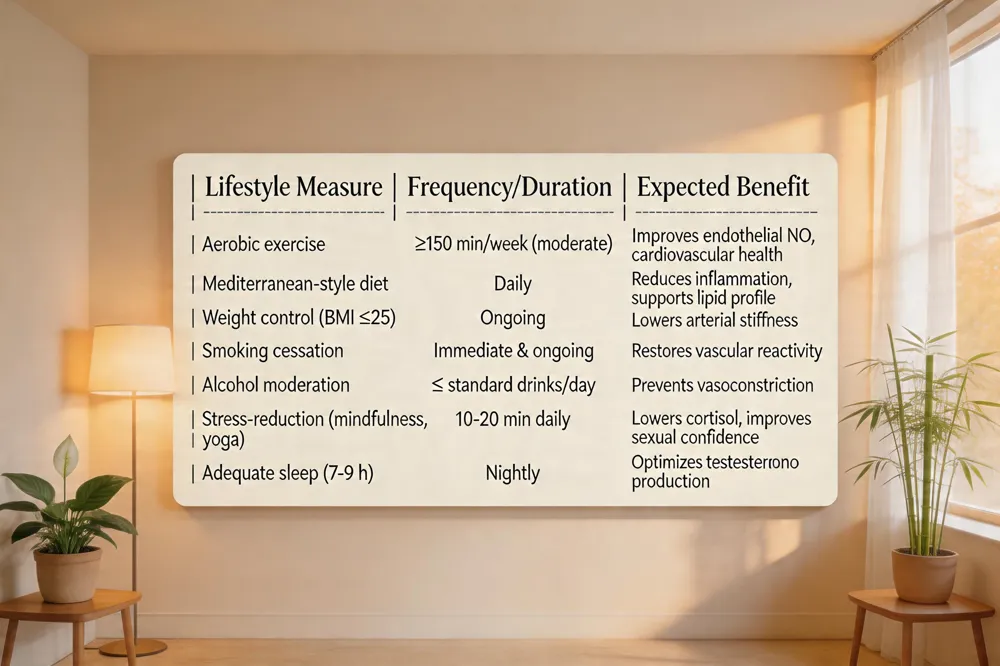
Regular moderate aerobic exercise—brisk walking, jogging, cycling or swimming for at least 30 minutes most days improves cardiovascular health, enhances endothelial function, and increases blood flow to the penis.
A heart‑healthy diet rich in fruits, vegetables, whole grains, lean proteins and omega‑3‑rich fish while low in processed foods, refined sugars and saturated fats supports hormone balance and reduces vascular risk.
Maintaining a healthy weight (BMI ≤ 25 kg/m²) and quitting smoking protect blood vessels and nerve pathways essential for erections, while limiting alcohol intake avoids its vasoconstrictive effects.
Stress‑reduction techniques such as mindfulness meditation, yoga, deep‑breathing exercises, and counseling can lower anxiety‑related sexual dysfunction.
Prioritizing 7‑9 hours of restorative sleep each night promotes optimal testosterone production and overall vitality.
Together, these lifestyle measures address the primary physical and psychological contributors to erectile dysfunction and can significantly improve erectile quality before or alongside medical therapies.
Psychological Factors and Counseling

[Performance anxiety] and [depression] are major contributors to erectile dysfunction (ED). Anxiety about sexual performance can trigger a self‑fulfilling cycle of inadequate erections, while [depressive] symptoms lower libido and diminish the neural signals needed for erection. [Relationship stress]—conflict, poor communication, or unmet expectations—also heightens anxiety and can directly impair sexual arousal. Addressing these psychosocial elements is essential; cognitive‑behavioral therapy (CBT) has demonstrated robust benefits. CBT helps men identify and reframe negative thoughts, develop coping strategies for anxiety, and improve communication skills with your partner. Studies consistently show that CBT, often combined with counseling or sex‑therapy, enhances erectile function scores and reduces reliance on medication, especially when the psychological component is prominent. Open dialogue with a qualified therapist, together with partner involvement, creates a supportive environment that mitigates performance pressure and promotes lasting sexual health.
Regenerative Medicine and Emerging Therapies
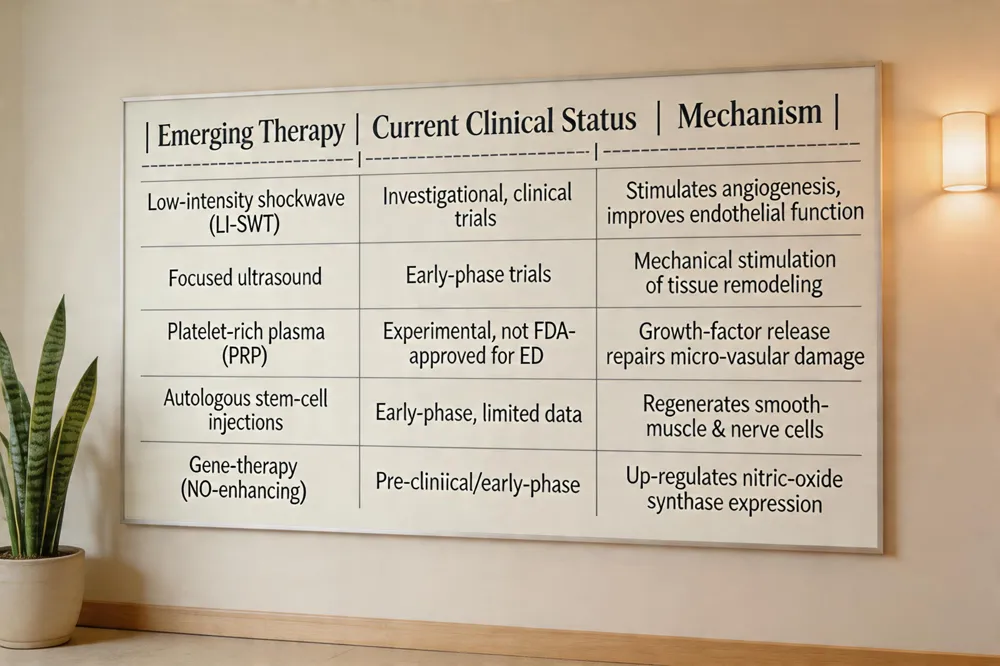
Low‑intensity shockwave therapy (LI‑SWT) and focused‑ultrasound modalities are being investigated as non‑invasive ways to improve penile blood flow. By delivering acoustic energy to the corpora cavernosa, they may stimulate angiogenesis and restore endothelial function, offering modest gains in men with mild vasculogenic erectile dysfunction. Clinical data are still emerging, and most guidelines list these techniques as investigational rather than first‑line treatments. Platelet‑rich plasma (PRP) and stem‑cell injections represent another frontier. PRP is harvested from the patient’s own blood, concentrated, and injected into penile tissue to release growth factors that could repair micro‑vascular damage. Autologous stem‑cell therapy aims to regenerate smooth‑muscle and nerve cells, potentially reversing structural causes of erectile dysfunction. Neither approach has been FDA‑approved for routine use; early‑phase studies show variable outcomes and raise concerns about standardization, dosing, and long‑term safety. For patients considering any regenerative option, enrollment in a well‑designed clinical trial is the safest path. Trials should include randomized, placebo‑controlled arms, validated outcome measures such as the International Index of Erectile Function, and clear reporting of adverse events. Participation enables access to cutting‑edge therapies while contributing to the evidence base that will determine whether these modalities become part of standard erectile‑dysfunction care.
Your Specialist at BeYounger Clinic

The leading physician for erectile dysfunction at BeYounger Clinic is Dr. Michael J. McGowan, MD. Dr. McGowan serves as the clinic’s chief male‑sexual‑health specialist and oversees all ED evaluations and treatments. He combines a physician‑led approach with regenerative‑medicine techniques to create personalized, medically supervised plans for each patient.
Comprehensive ED evaluation process – Under Dr. McGowan’s direction, a thorough health and sexual history is taken, followed by a focused physical exam and targeted laboratory tests (fasting glucose, lipid panel, thyroid‑stimulating hormone, and morning total testosterone). Vascular assessment may include penile Doppler ultrasound, while validated questionnaires such as the IIEF‑5 quantify severity. This systematic work‑up identifies diabetes, hypertension, dyslipidaemia, low testosterone, or medication effects—allowing early cardiovascular risk management.
Personalized treatment planning – Based on the diagnostic findings, Dr. McGowan tailors a multimodal regimen: lifestyle counseling (regular aerobic exercise, heart‑healthy Mediterranean diet, weight management, smoking cessation, stress reduction, first‑line oral PDE5 inhibitors with proper timing, pelvic‑floor (Kegel) training, and, when indicated, testosterone replacement. For men who do not respond to oral therapy, he offers non‑pharmacologic options such as vacuum erection devices, low‑intensity shockwave therapy, platelet‑rich plasma (PRP) injections, and, in refractory cases, surgical penile implants. Throughout, open communication with the patient and partner is emphasized to reduce anxiety, set realistic expectations, and optimize long‑term sexual health.
Curability and Sudden ED in Young Men
Erectile dysfunction (ED) is often reversible when the underlying cause is modifiable. Lifestyle factors—regular aerobic exercise, a heart‑healthy Mediterranean‑style diet, weight loss, smoking cessation, and limited alcohol—restore endothelial function and improve blood flow, which can eliminate mild to moderate ED without medication. Hormonal correction also matters; morning testosterone testing identifies hypogonadism, and testosterone replacement therapy restores libido and supports erections when levels are truly low.
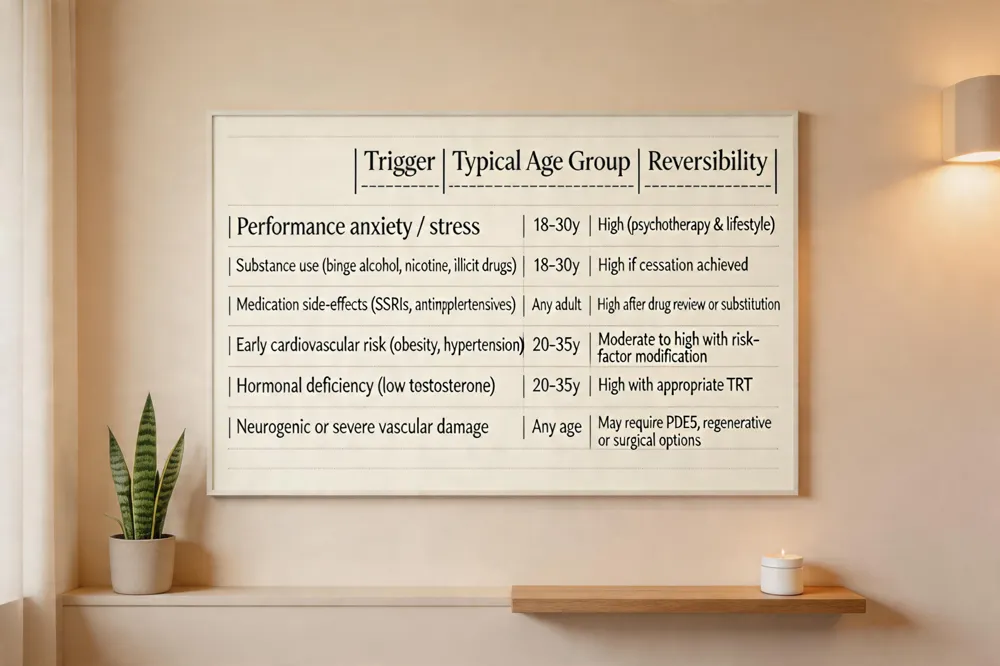
In men in their early twenties, specific triggers include: • Performance anxiety, stress, depression, or excessive pornography use that disrupt central nervous system signaling. • Substance use—binge drinking, nicotine, or illicit drugs—that acutely impairs vascular tone and nitric‑oxide production. • Medication side‑effects (e.g., certain antidepressants or antihypertensives) and untreated sleep apnea, which lower testosterone and damage vascular health.
Is erectile dysfunction curable? Yes, in many cases. When ED stems from reversible contributors such as lifestyle habits, hormonal imbalance, or medication effects, targeted changes often restore normal function. Permanent vascular or neurogenic damage may not be fully curable, but effective therapies—including PDE5 inhibitors, low‑intensity shockwave treatment, or penile implants—can provide reliable erections.
What causes sudden erectile dysfunction in a 21‑year‑old male? Acute ED at this age can arise from early cardiovascular risk (high blood pressure, rising glucose, obesity), low testosterone, stress‑related performance anxiety, excessive alcohol or drug use, and medication side‑effects. A comprehensive medical evaluation is essential to pinpoint the exact trigger and guide treatment.
Putting It All Together
In summary, the ten patient‑focused tips are: (1) take a thorough health and sexual history; (2) get a physical exam and basic labs (glucose, lipids, testosterone); (3) adopt heart‑healthy habits—regular aerobic activity, a diet rich in fruits, vegetables, whole grains, and lean protein, and maintain a healthy weight; (4) quit smoking and limit alcohol; (5) manage stress and address anxiety or depression through counseling; (6) discuss FDA‑approved PDE5 inhibitors and learn proper timing and dosing; (7) consider non‑pharmacologic options such as vacuum devices or pelvic‑floor (Kegel) exercises; (8) involve your partner in open communication; (9) review all medications for possible side‑effects; and (10) schedule regular follow‑up for ongoing monitoring.
If you’re ready for a tailored approach, BeYounger offers personalized, physician‑guided care that integrates lifestyle coaching, hormone evaluation, and cutting‑edge therapies.
Next steps: book a comprehensive evaluation, commit to the lifestyle changes above, and partner with your clinician to monitor progress, adjust treatments, and sustain long‑term sexual vitality.


